What if a patient with severe gingival inflammation does everything right—excellent oral hygiene, thorough scaling and root planing—yet the gums refuse to heal?
This is where plasma cell periodontitis, a rare and often overlooked condition, should be on every dentist’s radar.
Plasma cell periodontitis is not plaque-induced periodontal disease, yet it can look exactly like it. Because of this, many cases are misdiagnosed, leading to delayed treatment and frustration for both dentist and patient.
Clinical Presentation
A 32-year-old female patient presented with:
- Diffuse gingival inflammation
- Gingival enlargement
- A burning sensation in the gums
- Associated cheilitis


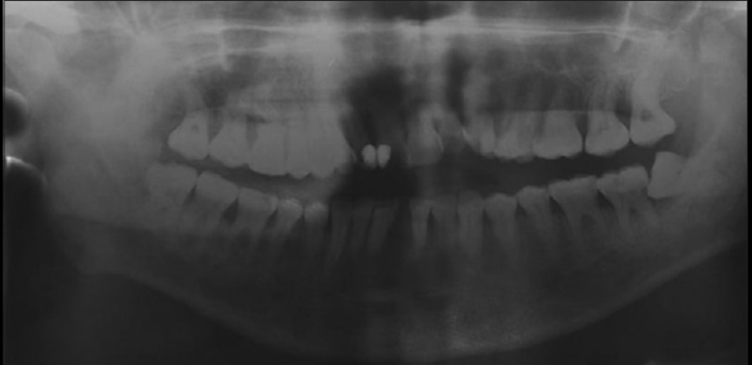
Periodontal examination revealed deep periodontal pockets and radiographic bone loss, suggesting chronic periodontal involvement. The patient had no relevant medical history and reported this as her first episode.
Diagnostic Challenges
Initial nonsurgical periodontal therapy, including scaling and root planing, resulted in limited improvement, which was inconsistent with typical plaque-related periodontal disease. Routine laboratory tests and imaging showed no systemic abnormalities.
Given the atypical response to treatment, a gingival and labial biopsy was performed.
Histopathological Findings
Microscopic examination revealed:
- Dense inflammatory connective tissue
- Predominant infiltration of plasma cells
- Features consistent with a benign, reactive process
These findings confirmed the diagnosis of plasma cell periodontitis with periodontal involvement.
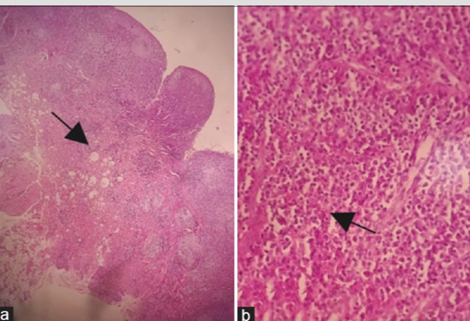
(a) Microscopic image showing gingival tissue with a dense inflammatory cell infiltrate (black arrow) (b) Microscopic image showing a polymorphic inflammatory infiltrate rich in plasma cells (black arrow) .
Possible Etiological Factors
The exact cause of plasma cell periodontitis remains unclear. However, proposed contributing factors include:
- Hypersensitivity reactions
- Exposure to spices, cinnamon, mint, or flavored toothpaste
- Cosmetic or oral hygiene products
- Possible reaction to bacterial antigens
This may explain the reduced response to mechanical therapy alone.
Management and Outcome
Treatment focused on both local and systemic control:
- Comprehensive periodontal therapy
- Systemic antibiotics (amoxicillin and metronidazole)
- Endodontic treatment of the affected tooth
- Reinforcement of oral hygiene measures
Clinical improvement was observed over follow-up visits, although healing progressed more slowly than in conventional periodontitis.
Clinical Relevance for Dentists
Plasma cell periodontitis should be considered when clinicians encounter:
- Persistent gingival erythema and enlargement
- Periodontal inflammation unresponsive to standard therapy
- Clinical findings disproportionate to plaque levels
In such cases, histopathological examination is essential to confirm the diagnosis and guide management.
Although rare, plasma cell periodontitis is an important differential diagnosis in non-responsive periodontal cases. Early recognition, biopsy, and a multidisciplinary approach can improve treatment outcomes and prevent unnecessary interventions.
Reference
Plasma cell periodontitis: A rare disease entity with unique clinical and histopathological features — A recent case report of plasmacytoid mucositis involving periodontal tissues, demonstrating plasma cell infiltration and periodontal involvement. PubMed
https://pubmed.ncbi.nlm.nih.gov/39411726/ PubMed