Orthodontic treatment has transformed millions of smiles, but every tooth movement comes with a biological response. While closing extraction spaces is a routine part of orthodontic practice, a new study suggests that the magnitude and pattern of incisor retraction may significantly influence the risk of external apical root resorption (EARR) in adult patients.
Published study provides valuable clinical insights that can help orthodontists plan safer and more predictable treatments, particularly in adults requiring premolar extractions.
Why Is This Study Important?
Premolar extraction remains a common treatment option for managing:
- Severe dental crowding
- Bimaxillary protrusion
- Lip incompetence
- Space requirements for facial profile improvement
Following extraction, the maxillary incisors are retracted to close the spaces and achieve ideal occlusion and facial esthetics. However, excessive orthodontic forces and prolonged tooth movement can place considerable stress on the root apex, increasing the risk of inflammatory root resorption.
This study aimed to determine whether the amount of incisor retraction and the type of tooth movement influence the severity of root resorption.
Study at a Glance
Researchers retrospectively evaluated 180 adult patients who underwent orthodontic treatment with extraction of at least two maxillary premolars.
Patients were divided into three groups based on the amount of upper incisor retraction:
- Group 1: Less than 4 mm
- Group 2: 4–8 mm
- Group 3: More than 8 mm
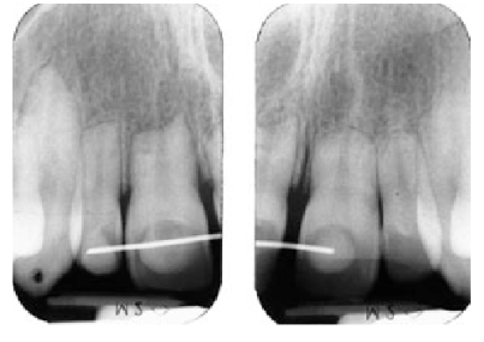
Root resorption was assessed using panoramic radiographs, while cephalometric analysis was used to evaluate skeletal changes and tooth movement patterns.
Major Findings
The results demonstrated a clear dose-dependent relationship between tooth movement and root resorption.
The researchers found:
- Greater maxillary incisor retraction resulted in significantly higher external apical root resorption.
- Patients with more than 8 mm of retraction experienced the greatest root shortening.
- Root-to-crown ratio decreased as retraction distance increased.
- Translation (bodily movement) appeared to produce more root resorption than uncontrolled tipping.
- Appliance type, apical displacement, and miniscrew anchorage also influenced the severity of resorption.
- Skeletal pattern showed no significant association with root resorption.
Clinical Significance for Orthodontists
Although mild root resorption is an accepted biological consequence of orthodontic treatment, excessive root shortening may compromise long-term tooth prognosis in susceptible patients.
The findings reinforce several important clinical principles:
- Plan extraction cases carefully before committing to large incisor retraction.
- Use controlled biomechanics to minimize stress at the root apex.
- Monitor root length with periodic radiographic evaluation, especially during prolonged treatment.
- Identify patients who may be at increased biological risk for root resorption.
- Discuss potential risks with patients during informed consent.
The Takeaway
Every millimeter of orthodontic tooth movement has biological consequences. This study reminds clinicians that achieving ideal esthetics should always be balanced with preserving the long-term health of the tooth and its supporting structures.
For orthodontists, understanding the relationship between incisor retraction and external apical root resorption is essential for delivering predictable, evidence-based care. As biomechanics and imaging technologies continue to evolve, future treatment protocols may further reduce this complication while maintaining excellent functional and esthetic outcomes.
Reference
Effect of incisor retraction magnitude and movement pattern on root resorption after premolar extraction in adults